|
Overview
While a slight amount of pronation is the proper means to absorb shock naturally, too much pronation (over-pronation) can potentially contribute to many maladies, which can sideline a runner. A foot that pronates excessively is one that continues to roll inward past a neutral position after the shock of impact has been absorbed. Uncorrected and repeated, this motion may lead to repetitive stress related injuries of the feet and legs. More times than not, the runner who over-pronates needs a shoe that reduces excess pronation and guides the foot along a neutral path.  Causes You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation. Symptoms Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven. Diagnosis You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.  Non Surgical Treatment The following exercises help retrain the foot and ankle complex to correct overpronation. Step Up and Over. This exercise is designed to integrate skills learned in the Duck Stand, Big Toe Pushdowns and Side Step with Opposite Reach exercises to mimic walking and even running. Using the gluteal muscles and big toe in tandem will prevent overpronation while moving back and forth over the BT in a more effective, balanced motion. Movement Directions. Stand with left foot on top of the BT dome. (Note: For added balance, the right foot can tap on the ground, if needed). Extend right foot backwards to the ground and drop hips into a lunge position. Make sure that the right arm rotates across the left leg (this will activate the gluteal muscles on the left side). Now, step through and over the BT into a front lunge with the right leg forward. While lunging forward, the torso and left arm now rotate over the right leg. Throughout the exercise, push big toe down into the BT. Perform 8 to 10 repetitions on both sides. Prevention Wear supportive shoes. If we're talking runners you're going to fall in the camp of needing 'motion control' shoes or shoes built for 'moderate' or 'severe' pronators. There are many good brands of shoes out there. Don't just wear these running, the more often the better. Make slow changes. Sudden changes in your training will aggravate your feet more than typical. Make sure you slowly increase your running/walking distance, speed and even how often you go per week. Strengthen your feet. As part of your running/walking warm up or just as part of a nightly routine try a few simple exercises to strengthen your feet, start with just ten of each and slowly add more sets and intensity. Stand facing a mirror and practice raising your arch higher off the ground without lifting your toes. Sit with a towel under your feet, scrunch your toes and try to pull the towel in under your feet. Sitting again with feet on the ground lift your heels as high as you can, then raise and lower on to toe tips. Overview
Growing pains are very common among physically active children ages 9 to 14. These growing pains or bone disorders are only temporary and have no long-term effects. Sever's disease, also known as calcaneal apophysitis, is a painful swelling and inflammation of the growth plate in the heel. Causes The pain of Severs usually occurs because of inflammation and micro-trauma to the growth plate of the heel bone. This can be caused by a sudden increase in activity, running on very hard surfaces, a growth spurt, tight muscles or feet that roll in. Symptoms The condition can be quite disabling and tends to affect those who are very busy with sporting activities. In the initial stages of the condition, most children displaying signs of Severs disease will tend to hobble or limp off the sports field or court and complain of sore heels near the end of activity. As the condition progresses, children may complain of pain during activity and in severe cases prior to sporting activities. Kids heel pain can be quite discouraging for active children but, early treatment can resolve this type of foot pain in children very quickly. Diagnosis X-rays are normal in Sever's disease, but your doctor will probably get X-rays to rule out other problems. Treatment consists of non-steroidal anti-inflammatory medications and use of a heel lift to relieve tension on the calcaneal apophysis. In more severe cases, phycical therapy consisting of modalities to relieve the pain, and stretching exercises may be helpful. In extreme cases, castings have been used. Non Surgical Treatment Treatment for Sever?s disease is mainly supportive, to stop inflammation and reduce pain. The condition will resolve on its own when the growth in the growth plate is complete, but until then, measures can be taken to resolve pain and discomfort. Applying ice to the painful or swollen areas on the foot may provide some short-term relief from pain and prevent further inflammation. Ice can be applied for about 20 minutes two or three times a day. Footwear that is too big, too small, or does not provide proper support can exacerbate the symptoms of Sever?s disease. Supportive footwear is important to prevent discomfort, especially in children who participate in sports and activities that take place on a hard surface (such as pavement or a basketball court). Shoes should also have adequate padding and not rub against the heel. In some cases, shoes that do not have heels (such as sandals) may be more comfortable to wear while the heel is healing, but care should be taken that the shoe provides proper support to the rest of the foot. Children with Sever?s disease should avoid going barefoot.Children with flat feet, high arches, or over-pronation may need treatment to resolve these underlying conditions. In many cases, an orthotic worn inside the shoe can help put the foot into a better alignment and provide relief to the foot or the arch. Children who are overweight or obese may be counseled to lose weight. Being overweight can contribute to the development of several conditions, including Sever?s disease. Resting the foot and discontinuing sports and other activities until the pain and stiffness is resolved may be recommended. In extreme cases, a walking boot or a cast might be used to completely immobilize the foot. A physical therapist may recommend stretching exercises for the muscles in the calf and the Achilles tendon. A stretching routine is usually done several times a day. Stretching these muscles can help improve strength and decrease the stress on the heel plate. Some physicians may recommend over-the-counter pain relievers such as ibuprofen or acetaminophen. Care must be taken when administering these medications to children, especially with acetaminophen, as overdoses are possible when using more than one medication containing acetaminophen. Aspirin should never be given to children. The utility of pain relievers in children must be weighed against their possible side effects. For small variations-less than an inch or so-shoe lifts can help equalize the length of the legs. In cases with more variation between legs, surgical solutions may be considered. Research indicates that targeted manual therapy techniques performed by a licensed physical therapist can help to reduce pain from Sever?s Disease and to improve muscle function. When the larger calf muscles and the smaller ankle and foot muscles become tight, this tightness can affect the mechanics of the ankle joint. Manual therapy includes both joint and muscle release techniques to restore optimal function to the calf, ankle, and foot muscles, and results can generally be achieved within a few months. Prevention Because there are several theories as to the actual cause of the disease, there is no definitive answer on prevention. Experts agree, though, that youth athletes can help minimize the risk of Sever's disease by maintaining good joint and muscle flexibility while engaging in sports or physical activities.
Overview
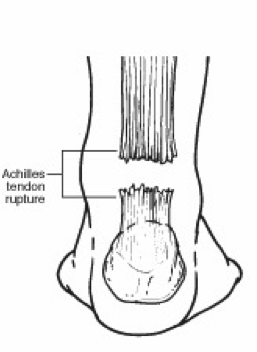 The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus. The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.Causes An Achilles tendon rupture is often caused by overstretching the tendon. This typically occurs during intense physical activity, such as running or playing basketball. Pushing off from the foot while the knee is straight, pivoting, jumping, and running are all movements that can overstretch the Achilles tendon and cause it to rupture. A rupture can also occur as the result of trauma that causes an over-stretching of the tendon, such as suddenly tripping or falling from a significant height. The Achilles tendon is particularly susceptible to injury if it is already weak. Therefore, individuals who have a history of tendinitis or tendinosis are more prone to a tendon rupture. Similarly, individuals who have arthritis and overcompensate for their joint pain by putting more stress on the Achilles tendon may also be more susceptible to an Achilles tendon rupture. Symptoms It happens suddenly, often without warning. There is often a popping sound when the tendon ruptures. The patient usually feel as if someone has kicked their heel from the rear, only to turn around to find nobody there. There is acute pain and swelling in the back of the heel due to bleeding from the tendon rupture. The patient will have difficulty walking as they cannot toe off without pain. This causes them to walk with a limp. Diagnosis Your doctor will ask you about your symptoms and examine you. He or she may also ask you about your medical history. Your doctor may ask you to do a series of movements or exercises to see how well you can move your lower leg. He or she may also examine your leg, heel and ankle and may squeeze your calf muscle to check the movement of your foot. You may need to have further tests to confirm if your tendon is torn, which may include the following. An ultrasound scan. This uses sound waves to produce an image of the inside of your leg. An MRI scan. This uses magnets and radio waves to produce images of the inside of your leg. Non Surgical Treatment There is no definitive protocol for conservative management. Traditionally, conservative treatment involved immobilisation in a cast or boot, with initial non-weight bearing. Recently, good results have been achieved with functional bracing and early mobilisation, and it is common to be immediately weight-bearing in an orthotic. Conservative management reduces the chance of complications, such as infection. There is a risk the tendon can heal too long and more slowly.  Surgical Treatment The surgical repair of an acute or chronic rupture of the Achilles tendon typically occurs in an outpatient setting. This means the patient has surgery and goes home the same day. Numbing medicine is often placed into the leg around the nerves to help decrease pain after surgery. This is called a nerve block. Patients are then put to sleep and placed in a position that allows the surgeon access to the ruptured tendon. Repair of an acute rupture often takes somewhere between 30 minutes and one hour. Repair of a chronic rupture can take longer depending on the steps needed to fix the tendon. Overview
Leg length discrepancy is a condition where the length of one leg is different than the other (shorter or longer) because of either or both a functional (muscle/posture) or structural (bone/cartilage) abnormality. In the specific a functional leg length occurs when your legs are the same, but another condition such as pelvic tilt or piriformis shortening creates the appearance of one leg being longer or shorter than the other. A structural leg length inequality it means that there is a true difference. Osteopaths, chiropractors and physiotherapist should be able to determine the degree of leg length inequality using visual inspection and manual tests.  Causes Leg length discrepancies can be caused by: hip and knee replacements, lower limb injuries, bone diseases, neuromuscular issues and congenital problems. Although discrepancies of 2 cm or less are most common, discrepancies can be greater than 6 cm. People who have LLD tend to make up for the difference by over bending their longer leg or standing on the toes of their shorter leg. This compensation leads to an inefficient, up and down gait, which is quite tiring and over time can result in posture problems as well as pain in the back, hips, knees and ankles. Symptoms The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding. Diagnosis The evaluation of leg length discrepancy typically involves sequential x-rays to measure the exact discrepancy, while following its progression. In addition, an x-ray of the wrist allows us to more carefully age your child. Skeletal age and chronological age do not necessarily equal each other and frequently a child's bone age will be significantly different than his or her stated age. Your child's physician can establish a treatment plan once all the facts are known: the bone age, the exact amount of discrepancy, and the cause, if it can be identified. Non Surgical Treatment A personalized approach to leg length discrepancy treatment works best for each patient. Your child's doctor will consider many factors when deciding on a course of treatment for this condition. Such factors can include your child's age, extent of the leg length discrepancy, medical history, how your child tolerates certain treatments and procedures, your child's health and prognosis, growth rate, and parental preferences. There is no cookie cutter treatment for each child, or even each centimeter of leg difference. Once all of these factors have been carefully considered, your child's physician will come up with an appropriate course of care. In situations of a very small leg length discrepancy, no treatment, only periodic medical evaluation, may be necessary.  Surgical Treatment The type of surgery depends on the type of problem. Outpatient procedures may be used to alter the growth of the limb. This is often done through small incisions. If an outpatient procedure is done, your child can continue with most regular activities. Other times, surgery may be very involved and require the use of an external device that is attached to the limb with pins and wires. This device may be left on for months to correct the deformity or lengthen the leg. If this type of surgery is required, your child will be making weekly visits to Cincinnati Children's.
Overview
Adult-acquired flatfoot is a challenging condition to treat. It is defined as a symptomatic, progressive deformity of the foot caused by loss of supportive structures of the medial arch. It is becoming increasingly frequent with the aging population and the obesity epidemic. Patients commonly try to lose weight by exercising to improve the condition. This often leads to worsening of symptoms and progression of the disorder. Early recognition of this complex disorder is essential, if chronic pain and surgery are to be avoided.  Causes Causes of an adult acquired flatfoot may include Neuropathic foot (Charcot foot) secondary to Diabetes mellitus, Leprosy, Profound peripheral neuritis of any cause. Degenerative changes in the ankle, talonavicular or tarsometatarsal joints, or both, secondary to Inflammatory arthropathy, Osteoarthropathy, Fractures, Acquired flatfoot resulting from loss of the supporting structures of the medial longitudinal arch. Dysfunction of the tibialis posterior tendon Tear of the spring (calcaneoanvicular) ligament (rare). Tibialis anterior rupture (rare). Painful flatfoot can have other causes, such as tarsal coalition, but as such a patient will not present with a change in the shape of the foot these are not included here. Symptoms Often, this condition is only present in one foot, but it can affect both. Adult acquired flatfoot symptoms vary, but can swelling of the foot's inner side and aching heel and arch pain. Some patients experience no pain, but others may experience severe pain. Symptoms may increase during long periods of standing, resulting in fatigue. Symptoms may change over time as the condition worsens. The pain may move to the foot's outer side, and some patients may develop arthritis in the ankle and foot. Diagnosis Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing. Non surgical Treatment This condition may be treated with conservative methods. These can include orthotic devices, special shoes, and bracing. Physical therapy, rest, ice, and anti-inflammatory medication may be prescribed to help relieve symptoms. If the condition is very severe, surgical treatment may be needed.  Surgical Treatment If conservative treatments don?t work, your doctor may recommend surgery. Several procedures can be used to treat posterior tibial tendon dysfunction; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your individual case. Surgical options include. Tenosynovectomy. In this procedure, the surgeon will clean away (debride) and remove (excise) any inflamed tissue surrounding the tendon. Osteotomy. This procedure changes the alignment of the heel bone (calcaneus). The surgeon may sometimes have to remove a portion of the bone. Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon. Lateral column lengthening, In this procedure, the surgeon places a small wedge-shaped piece of bone into the outside of the calcaneus. This helps realign the bones and recreates the arch. Arthrodesis. This procedure welds (fuses) one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and prevents the condition from progressing further. |
